COLOUR-FLOW DUPLEX INVESTIGATION IN SUPERFICIAL VENOUS INSUFFICIENCY OF THE LOWER LIMBS
Cavezzi Attilio M.D. cavezzia@insinet.it
SUMMARY
Colour-flow duplex imaging (CFDI) investigation has become the cornerstone of the diagnostic-therapeutic approach to varicose vein disease; morphologic and haemodynamic information may be safely collected with great accuracy by means of duplex (colour-flow) exploration, reducing greatly the necessity of invasive contrastographic means.
In the last few years it has been possible to highlight a few "new" patterns of saphenous incompetence: a) long and short saphenous vein are very rarely (3% of the affected limbs in cases of LSV) insufficient from the junction to the ankle, a segmental reflux being more common, b) in cases of long saphenous reflux, the sapheno-femoral junction is competent (no reflux from common femoral vein) in about 30% of the patients, while several extra-junctional reverse flows are possible, c) in primary varicose veins perforating veins of the leg have mainly a re-entry role, even if enlarged and with bi-directional flow.
In the field of superficial venous disease, CFDI permits also: a) the clarification of the vast majority of the complex patterns of recurrent varices, b) the definition and the monitoring of the superficial venous thrombosis, finally c) improvement in our knowledge of the minor varicosities and finally even d) the possibility to guide a safer and more precise sclerotherapic session (ultrasound guided sclerotherapy).
Whatever the therapeutic plan may be, the treatment of varicose vein disease must be guided by a correct diagnostics, principally relying upon colour-flow-duplex imaging: the true gold standard for this kind of vascular disease.
 |
 |
INTRODUCTION
Ultrasound diagnostics, which began with doppler c.w. and then duplex scanning (DS), have into the last few years developed into colour-flow duplex imaging (CFDI), which guarantees better anatomical and functional accuracy.
Such safe, non invasive, and reliable equipment has progressively revolutionized all the varicose vein disease diagnostics and has greatly improved surgery and sclerotherapy (1). Nowadays DS or CFDI may (and must) guide the phlebologist's therapeutical steps, when treating trunk varicose veins or smaller varicosities of the lower limbs. By means of this kind of examination it is possible to collect several, precious anatomic information about the different characteristics of the superficial venous system (SVS), the deep venous system (DVS) and the perforating veins (PV) of the lower limb.
Alongside morphological information, it is possible to study the haemodynamics of the normal and pathologic veins of the lower limbs. The B-mode B/W image, coupled with the pulsed wave doppler beam (as in DS), allows us to investigate the different patterns of the venous flows; finally superimposing of colour flow imaging (as in CFDI) contributes to the creation of a true map of the varicose disease, facilitating the examination (even more so in obese, edematous limbs) and making it more accurate.
The CFDI has become the definitive gold standard for the diagnosis of lower limb varicose veins (and also of deep venous thrombosis, as demonstrated in most of the latest studies...); other complementary methods, such as plethysmographies, phlebodynamometry, can complete the diagnostic pathway of the patient, reaching a higher degree of understanding of specific venous disorders.
PRINCIPAL REMARKS OF COLOUR-FLOW DUPLEX IMAGING INVESTIGATION IN VARICOSE VEIN DISEASE
Basically what we require from the ultrasonographic investigation in cases of superficial venous disease is to know the patency and continence of the deep and superficial venous system and the state of perforating veins.
First of all Duplex scanning or CFDI may detect deep vein thrombosis (easily in the femoro-popliteal region, with good adequacy in the calf and abdominal sites), or its sequelae, such as thrombotic lesions all along the vein walls and, especially, deep venous valvular incontinence.
After this first important investigation of the DVS, the examination takes into account the SVS changes. All the superficial veins and the perforators are quite easy to visualize, and it is useful to localize and exactly qualify their confluences, valves, abnormalities, diameters, courses, sorrounding structures etc. The echographic examination is followed by the fundamental haemodynamic exploration, managed by the doppler spectral analysis (duplex) and/or by colour flow scanning.
The study of long and short saphenous vein (LSV and SSV respectively) is the most important moment of the diagnostic stage. Normal cephalad flow or reverse flow must be carefully investigated.
A true reflux from DVS to SVS may be evident in the sapheno-femoral junction (SFJ), or in the confluence of the SSV into the DVS (which is mainly , but not always, located in the popliteal region). By means of Valsalva's manoeuvre and especially through a compression-release of the distal part of the extremity, the 7.5 MHz (or 10 MHz) probe may reveal the reflux.
From this exploration we may notice how the reflux along the LSV is mostly (97% of the cases in a recent personal series of 225 incompetent LSVs of patients who underwent stripping and phlebectomy operation (2)) limited to the thigh or to the upper-medium third of the leg (just above or below Boyd's perforator). This means that the most peripheral portion of the long saphenous vein is almost always "healthy", that's why the short, segmental stripping of the LSV has become the most correct surgical procedure, abandoning the "invasive" and useless groin-to-ankle stripping.
In fact CFDI exploration shows that all the visible varicose veins of the thigh, and the vast majority of the varicose veins of the leg, belong to the saphenous tributaries, not affecting the LSV trunk, which runs deeper, into the duplication of the fascia (3) or between the superficial and deep fascia(4).
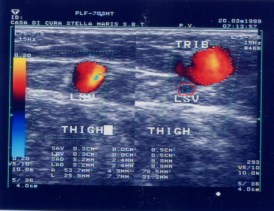
Apart from this "typical" condition, the ultrasonographic examination (especially with the help of colour-flow imaging) may highlight different pathological haemodynamic patterns. For example it is very common (30-35% of the patients in a few recent studies (5) (6), and 29% in our personal experience (7)) to find a reflux in the LSV without incompetence of the junction.
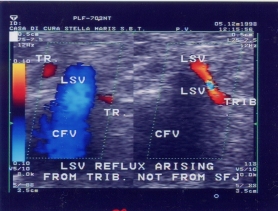
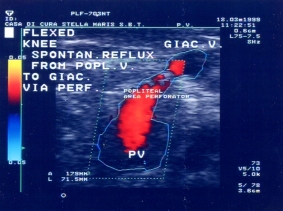
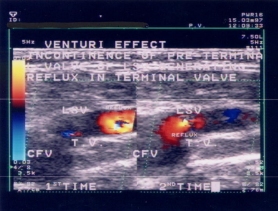
Among these extra-junctional reverse flows of the LSV we can mainly see: a) saphenous trunk isolated incompetence (pre-terminal valve incontinence, but continence of the terminal valve), b) pelvic-perineal reflux towards the LSV, c) retrograde flow in the peripheral saphenous tributaries (this seems to be the first stage of the varicose vein disease, which later affects the junction itself , mainly because of Venturi's effect (8)), d) true reflux from thigh or popliteal perforators, e) ascending reflux to LSV from SSV, via Giacomini's vein, due to DVS postural-functional compression and obstructed outflow (9).
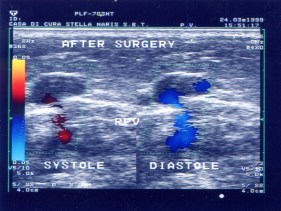
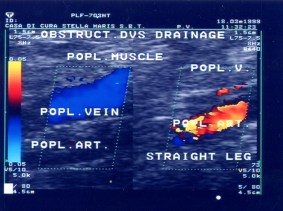
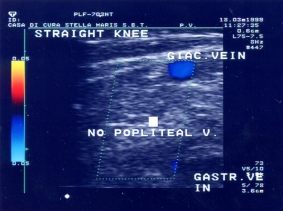
This last finding deserves special attention, as it seems not to be a rare abnormality. In fact postural muscular-ligamentous compression on the gastrocnemius-popliteal-femoral veins are sometimes evident, in the sense of a diverted flow from DVS to SVS, in order to bypass the obstructed (constricted) deep outflow. So blood may have an ascending SYSTOLIC (not diastolic…) reflux from DVS to saphenous axes, often using Giacomini's vein as intermediary conduit.
Another important part of the ultrasound investigation for the varicose vein diagnostics is the study of the perforating veins. In these last few years there has been a careful review of the role played by the perforators in the superficial venous disease (10) (11) (12). Through colour superimposition and doppler exploration, even enlarged PV (having diameter more than 2-3 mm) have often been tested as continent. In cases of primary varicose veins, whenever the flow in the PV is bi-directional (from SVS to DVS and vice-versa), the balance between these two kinds of flow is in favor of the re-entry of the blood towards the DVS, and this has been proven to be true in the majority of the perforators in the leg.
Objectively, we can also find true incompetent PV, mainly in the thigh region and in a small number of patients, which have reflux during the muscular diastolic (release) phase, and which may have an important role in the pathophysiology of varicose veins disease. But on the other hand, in the leg most of the PVs have a preminent re-entry function to DVS: in fact CFDI shows how the majority of the perforators have a short and limited pathological reflux from DVS to the SVS (that is to the varicose veins) during the muscular systole; whereas during the diastolic phase (calf muscle relaxation) these PVs aspirate, physiologically normal..., a large amount of blood to the DVS. These re-entry perforators represent an important finding to search for, in case of a surgical or sclerotherapeutic plan(13).
From this latest ultrasonographic confirmation of old Bjordal's (14), Tibb's (15) and even Perthes' studies about the utility and the "rare" malfunction of these venous structures, we may understand how the relative treatment of perforating veins should become more and more conservative....
Approaching varicose recurrence is not always easy, both from the diagnostic side and from the therapeutic point of view. Duplex scanning and CFDI are able to discover all the escape-points ( or the most important ones) which generate the recurrent varicose veins. Mainly they arise from (7): a) completely intact and unoperated saphenous junction, b) long saphenous stump with incontinent saphenous tributary or c) with accessory saphenous vein, d) pelvic-perineal refluxes (often arising from gonadal veins), e) reverse flows from abdominal subcutaneuos veins, f) new (or "old") incompetent perforators, g) peripheral incompetent saphenous side branches, h) extra-saphenous veins , i) neovascularization, l) enlarged branches directly coming from common femoral vein.
All of these patterns concerning superficial venous insufficiency may be currently clarified by a careful duplex or, better, colour-duplex exam.
We may not forget, however, that our lack of knowledge about the aetiology of primary varicose veins, may make any treatment of this disease far from perfect.... (a few relapses, as for the pelvic refluxes and the popliteal perforators, are even "physiological", we could say...).
The most recent technological facilities have furthermore enebled the study of the most superficial venous network, up to the tiniest capillaries (16). Through high-frequency probes, we can obtain information regarding the minor varicosities (reticular varices and telangiectasias) of the lower limb; this recent application has mainly a speculative-scientific purpose, but these haemodynamic findings may contribute to the comprehension and treatment of these cosmetic disorders. Concerning this argument it is becoming evident that many of these minor varicosities may arise from an obstructed drainage toward the deeper veins (i.e. towards the subcutaneous plexus, PV, DVS, saphenous axes), not due to a reflux from these deeper veins (17).
One of the most common complications of varicose veins disease is varicophlebitis; in the presence of this superficial thrombosis the duplex or CFDI investigation can localize the upper part of the thrombus, evaluating its eventual extension to the DVS via perforators or via saphenous junctions, and finally monitoring the process. In this way the surgical or conservative therapeutic options are better discriminated and guided.
One last remark about the importance of colour-flow duplex scanning in phlebology is the recent (1989) introduction of the ultrasound-guided sclerotherapy (or echosclerotherapy). This consists of injecting a sclerosing agent into an incompetent vein under ultrasound guidance. By means of this last step, duplex and CFDI, after improving greatly the diagnostic approach, have finally entered the world of venous therapy itself.
CONCLUSIONS
We could say that phlebology and specifically varicose vein disease has undergone a kind of revolution in the diagnostic-therapeutic approach in the last 10-20 years, and the main protagonist of this revolution is (colour-flow) duplex imaging technology.... Ever more ultrasonographic findings are continuously updating our knowledge about superficial venous insufficiency; phlebologists of all over the world are definitively utilizing this powerful diagnostic instrument, receiving irreplaceable information for a better comprehension of the disease, and finally for an improvement in the therapeutic act.
Apart from the limits related to the quality of the equipment, in the end we have to underline the greatest limitation of the duplex or CFDI examination: it is an operator-dependant diagnostics, which is based on the experience and capability of the physician, who has to see what machine only helps to see...
BIBLIOGRAPHY
1) Schadeck M. Duplex and Phlebology. Gnocchi Ed., Napoli 1994
2) Cavezzi A., Frullini A., Long saphenous vein one-day surgery: relationship between haemodynamics and treatment. Abstr. XIII World Congr. of Phlebol., Sydney 1998: 93
3) Lemasle Ph., Baud J.M., Lefebvre-Villardebo M., Uhl J.F. Proposition d'une définition échographique de la grande saphčne et des saphčnes accessoires ŕ l'étape crural. Phlébologie 1996. 49; n.3: 279 - 86
4) Caggiati A., Ricci S. The long saphenous vein compartment. Phlebology 1997; 12: 107-111
5) Pieri A:, Vannuzzi A., Duranti A., Vin F., Caillard Ph., Benelli L., Michelagnoli S., De Saint-Pierre G. Rňle central de la valvule pré-ostiale de la veine saphčne interne dans la genčse des varices tronculaires des membres inférieurs Phlébologie 1995. 48; n.2 : 227-29 plus ERRATA Phlébologie 1995. 48. n. 4: V, VI
6) Cavezzi A. Long saphenous vein and perforating veins haemodynamics: "new" echo-colour-doppler patterns Abstr. XIII World Congr. of Phlebol., Sydney 1998: 109
7) Cavezzi A. Diagnostic de l'insuffisance veineuse superficielle des memmbres inferieurs par echo-doppler-couleur . Phlébologie (in press)
8) Creton D. Classification des sur 607 echo marquages: aspect evolutif de la maladie variqueuse Phlebology '95 D. Negus et als. ed. suppl.1. London Springer-verlag, 1995: 160-63
9) Pieri A., Vannuzzi A., Duranti A., Michelagnoli S., Marcelli F., Santini M., Somigli L., Ludovici M., Caillard Ph., Vin F. La valvule pré-ostiale de la veine saphčne externe. Phlébologie 1997. 50; n. 3: 343-350
10) Cappelli M., Molino Lova R:, Ermini S., Zamboni P. Fondamenti di emodinamica ed ultrasonografia venosa, pagg. 29-50 in "La chirurgia conservativa del sistema venoso superficiale", Zamboni P., CELI ED., Faenza 1996
11) Franceschi C. Physiopathologie hémodynamique de l'insuffisance veineuse des membres inférieurs, pagg.19-53 in "Chirurgie des veines des membres inférieurs", Kieffer, AERCV Ed., Paris 1996
12) Cappelli M., Ermini S., Turchi A., Bono G. Consideration hémodinamique sur les perforantes. Phlébologie 1994; 47, 4 : 389-93
13) Zamboni P. La chirurgia conservativa del sistema venoso superficiale CELI Ed., Faenza 1996
14) Bjordal R.I. Circulation patterns in incompetent perforating veins in the calf and in the saphenous system in primary varicose veins. Acta Chir. Scand. 1972; 138:251-61
15) Tibbs J.D:, Fletcher E.W. Direction of flow in superficial veins as a guide to venous disorders in lower limbs. Surgery, 1983; 6: 758-67
16) Somjen G.M., Ziegenbein R:, Johnston A.H., Royle J.P. Anatomical examination of leg telangiectases with dupex scanning. J.Dermatol. Surg. Oncol. 1993; 19: 940-45
17) Cavezzi A. Echo-colour-doppler findings in varicosities (reticular varices and telangiectasias) haemodynamics Abstr. 17° reun. Soc. Europ. Phlebect., Geneve 1997, pag.26